
Horse Health
Advice is given as a guide only and must not be relied upon. Please consult your vet for all equine medical matters.
Equine vets in the Charente Horse Group area: EquiSyn - Dr Sophie Lanniel - La Garde, 16260 Chasseneuil-sur-Bonnieure. T: 06 07 04 67 29, E: [email protected]. Surgery T: 05 45 92 32 87. Equipped with digital radiograph, ultrasound, endoscopy, blood analysis. Arcamvet - Dr Alexandre Richoux, T: 06 63 80 36 62, E: [email protected]. |
Piroplasmosis
Anaplasmosis
Lyme disease
Colic
Laminitis
Atypical Myopathy
Leptospirosis
Euthanasia and body disposal
RESPE
Medicines
Blood testing
Anaplasmosis
Lyme disease
Colic
Laminitis
Atypical Myopathy
Leptospirosis
Euthanasia and body disposal
RESPE
Medicines
Blood testing
Piroplasmosis
|
Summary
Equine Piroplasmosis (EP) is a blood borne disease carried by ticks that in the acute form can cause hemolytic anaemia, fever, weight loss, jaundice, colic, diarrhoea, liver damage, abortion and even death. It is present throughout France. Acute disease mostly occurs in naive horses that have moved from an area without EP (e.g. the UK) to an area where EP is endemic (like France). Diagnosis is now mostly by blood slide and PCR. Treatment for infected horses is 2 to 4 intra-muscular injections of Imidocarb (called Carbesia in France), depending on whether the aim of treatment is to eliminate just the clinical signs of disease or the parasitic infection (which may not be desirable in areas where EP is endemic), plus good nursing, diet, and supportive care in severe cases. Iron should not be supplemented to horses with piroplasmosis. Horses gain life-long immunity following infection (as long as low levels of infection remain). The best way to prevent piroplasmosis is to prevent ticks feeding on a horse, by checking horses every day for ticks and removing ticks if found (a Tire-Tique is good for removing ticks). and/or using an insect repellent, and where possible avoiding long grass/plants and bushes. |

|
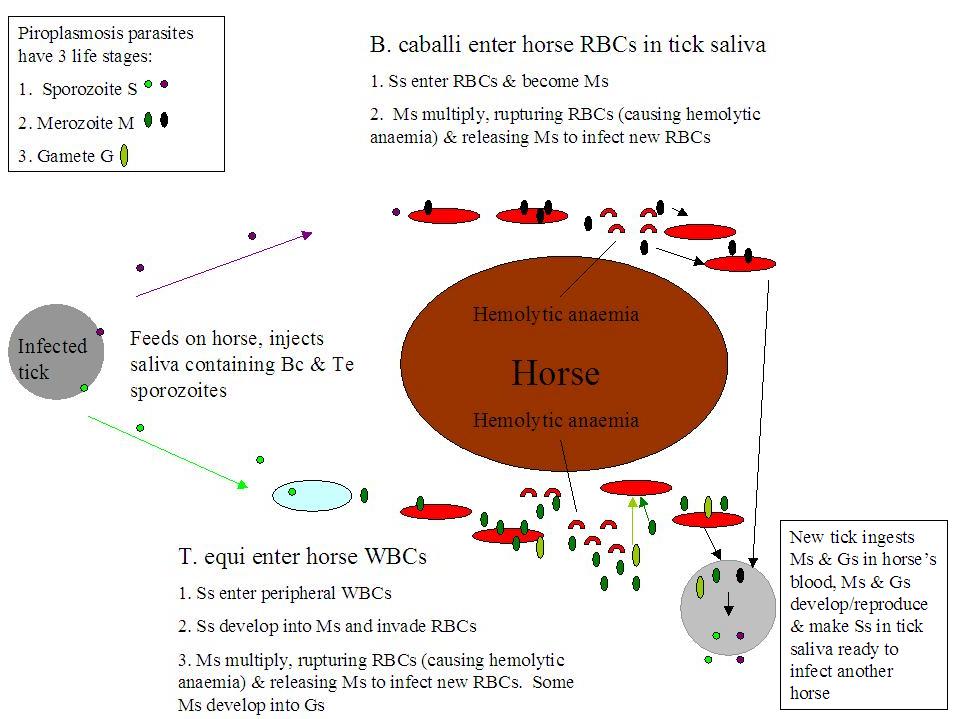
Equine piroplasmosis: life cycle of Babesia caballi and Theileria equi during tick transmission.
WBC = white blood cell
RBC = red blood cell
What is Equine Piroplasmosis (EP)?
Equine piroplasmosis describes infection by either or both of 2 protozoan (single-celled animal) parasites: Babesia caballi (B. caballi) and/or Theileria equi (T. equi). EP is sometimes called Babesiosis (infection by B. caballi alone) or Theileriosis (infection by T. equi alone), but the clinical signs of both diseases are so similar that equine piroplasmosis has become the blanket term to cover both infections. Generally infection with T. equi causes a more severe clinical disease. Feeding ticks pick up the parasites from an infected horse and inject them in their saliva into an uninfected ("naive") horse. The parasites can also be spread by contaminated blood, e.g. on needles, surgical instruments/dental tools or by blood transfusion. Once a tick is infected with the parasite, it can pass the infection to its offspring, so generations of ticks can transmit the disease without having to find another infected host (B. caballi only). Once inside the horse, the parasites invade the red blood cells (RBCs), where they multiply, causing the infected RBCs to rupture and more RBCs to be infected. In addition, RBCs are identified as contaminated and destroyed as they pass through the spleen, and the spleen destroys some uninfected RBCs too. This destruction of RBCs causes hemolytic anaemia (anaemia is described as hemolytic when RBCs are destroyed earlier than normal).
Clinical signs
Some horses become infected with equine piroplasmosis without showing any clinical signs (asymptomatic carriers), others show acute or chronic signs of the disease. The acute form can be mild and pass quickly, or can cause severe illness. It takes 10 to 30 days for a horse to show signs of acute piroplasmosis after being infected by a tick.
Signs of acute piroplasmosis often start with:
- Fever/above normal temperature (often exceeds 40'C). The horse's normal temperature is 37.5 to 38.5'C (although it has recently been found that individual differences mean that you should know your horse's normal temperature). For how to take the temperature see: How to take a horse's temperature - BHS. Note that it is worth spending a bit of extra money on a thermometer that beeps when ready, and that only takes 5 to 10 seconds.
- Going off feed/inappetence/anorexia, leading to weight loss.
- Lethargy.
- General malaise/being "not quite right".
- Increased heart rate (should be 28 to 44 beats per minute) and respiration rate (should be 8 to 16 breaths per minute). For how to take the heart rate and respiration rate, see: How to take a horse's pulse and respiratory rate - BHS (the video shows how to use both a stethoscope and the mandibular pulse for the heart rate. Remember you can also use the digital pulse in the fetlock or pastern).
- Mild colic (which may be followed by diarrhoea)
- Constipation (small dry dung or reduced passing of dung) (which may be followed by diarrhoea)
- Diarrhoea
- Peripheral oedema - swelling, particularly of the legs and/or below the belly
- Weakness in the hind end/swaying/ataxia, possibly seizures
- An enlarged spleen (this may be felt on rectal examination).
- Hemolytic anaemia - (the form of anaemia cased when red blood cells are destroyed earlier than they should be - in piroplasmosis the parasites cause RBCs to rupture and the spleen destroys infected RBCs). Hemolytic anaemia causes:
- Weakness,
- Blood in the urine (hemoglobulinuria - blood looks darker than normal/reddish/brown),
- Jaundice (technically called icterus) - yellow colour to the mucous membranes (eyelids, gums) (mucous membranes may also be pale due to anaemia),
- Petechiae (tiny red/purple dots) may be seen on the mucous membranes (gums, eyelids) (due to thrombocytopenia or low platelets).

B. caballi infected horse showing pale sclera (from Osman 2016)
|

B. caballi infected horse showing icteric sclera (from Osman 2016)
|
In more severe cases complications can include
Signs of chronic piroplasmosis are usually non-specific and include weakness, lethargy, poor performance/exercise intolerance, loss of appetite, weight loss, loss of condition, poor hair coat, transient fever and hemolytic anaemia. The spleen may be enlarged on rectal examination.
- liver failure, kidney damage/acute renal failure, secondary infections e.g. pneumonia, and systemic inflammatory response syndrome.
- Pregnant mares can pass piroplasmosis to the foetus, causing abortion and birth of stillborn foals. Infected live foals may develop clinical signs quickly, including anaemia and jaundice, or not show clinical signs and become healthy carriers.
Signs of chronic piroplasmosis are usually non-specific and include weakness, lethargy, poor performance/exercise intolerance, loss of appetite, weight loss, loss of condition, poor hair coat, transient fever and hemolytic anaemia. The spleen may be enlarged on rectal examination.
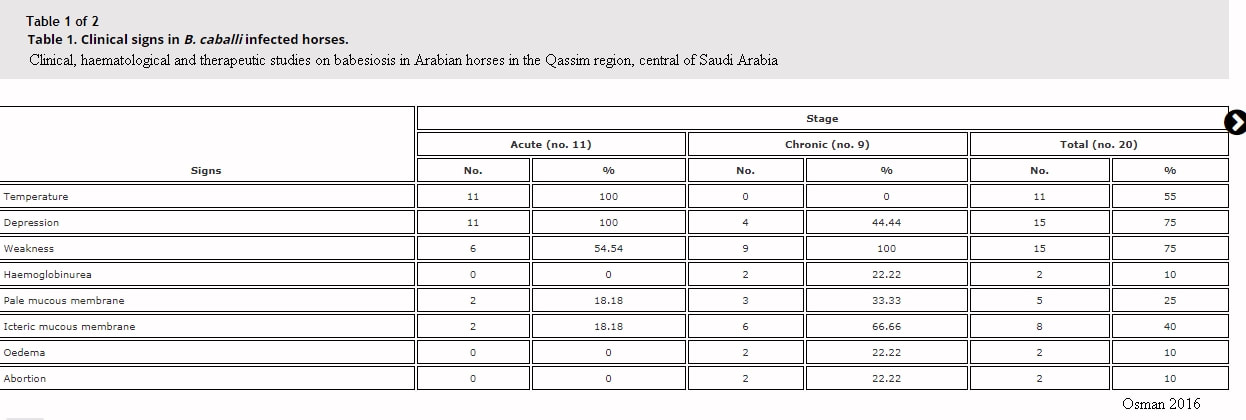
Clinical signs recorded in acute and chronic cases of infection with B. caballi in Saudia Arabia
Diagnosis
Diagnosis of equine piroplasmosis consists of specifically looking for parasitic infection - blood smear under the microscope and/or sending off blood for PCR and/or serological testing, supported by CBC (complete blood count) and biochemistry findings (CBC and biochemistry will usually be run by your vet so results should be available quickly). Normalization of the CBC may be a good indicator of response to treatment, and biochemistry should be monitored until liver and kidney enzymes are normal.
Complete Blood Count (CBC)
Anaemia is diagnosed by below normal red blood cell count (GR/hematies), haemoglobin (Hb/hemoglobine) and PCV/hematocrit (Hte/hematocrite) (in brackets are names that you might see on French blood test results). PCV can be as low as 10% but rarely decreases below 20%.
The anaemia is initially normocytic (MCV is normal), then becomes macrocytic (MCV is high).
MCH and MCHC are variable (will generally increase but may decrease)
Thrombocytopenia (decreased platelets) is often seen.
White blood cells and fibrinogen vary depending on the stage of infection and severity.
Diagnosis of equine piroplasmosis consists of specifically looking for parasitic infection - blood smear under the microscope and/or sending off blood for PCR and/or serological testing, supported by CBC (complete blood count) and biochemistry findings (CBC and biochemistry will usually be run by your vet so results should be available quickly). Normalization of the CBC may be a good indicator of response to treatment, and biochemistry should be monitored until liver and kidney enzymes are normal.
Complete Blood Count (CBC)
Anaemia is diagnosed by below normal red blood cell count (GR/hematies), haemoglobin (Hb/hemoglobine) and PCV/hematocrit (Hte/hematocrite) (in brackets are names that you might see on French blood test results). PCV can be as low as 10% but rarely decreases below 20%.
The anaemia is initially normocytic (MCV is normal), then becomes macrocytic (MCV is high).
MCH and MCHC are variable (will generally increase but may decrease)
Thrombocytopenia (decreased platelets) is often seen.
White blood cells and fibrinogen vary depending on the stage of infection and severity.
Biochemistry
Biochemistry changes may include:
decreases in: total protein, perhaps also albumin
increases in: bilibrubin, liver enzymes (AST, GGT, ALP, perhaps also LDH), CK and perhaps also urea. (Increased bilirubin can be an indicator of hemolytic anaemia. Raised liver enzymes may be because of reduced blood flow to the liver).
Biochemistry changes may include:
decreases in: total protein, perhaps also albumin
increases in: bilibrubin, liver enzymes (AST, GGT, ALP, perhaps also LDH), CK and perhaps also urea. (Increased bilirubin can be an indicator of hemolytic anaemia. Raised liver enzymes may be because of reduced blood flow to the liver).
|
|
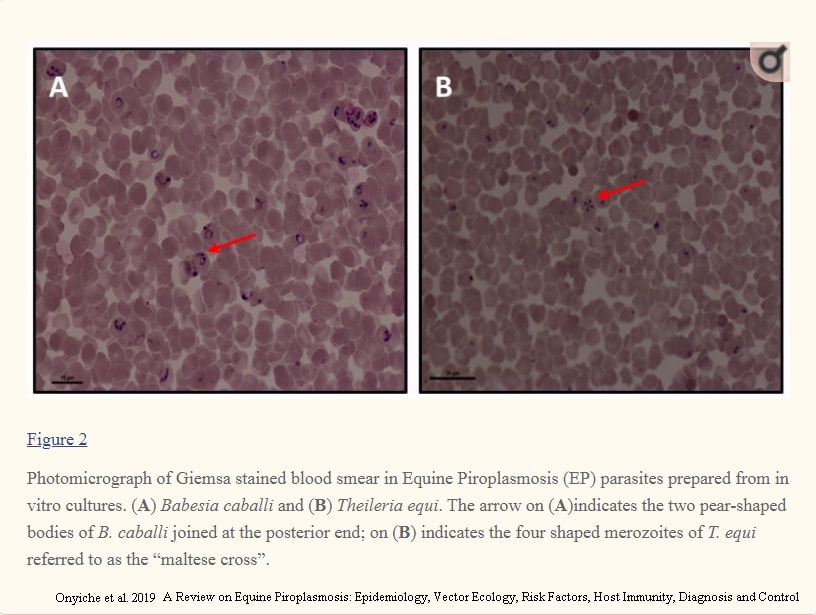
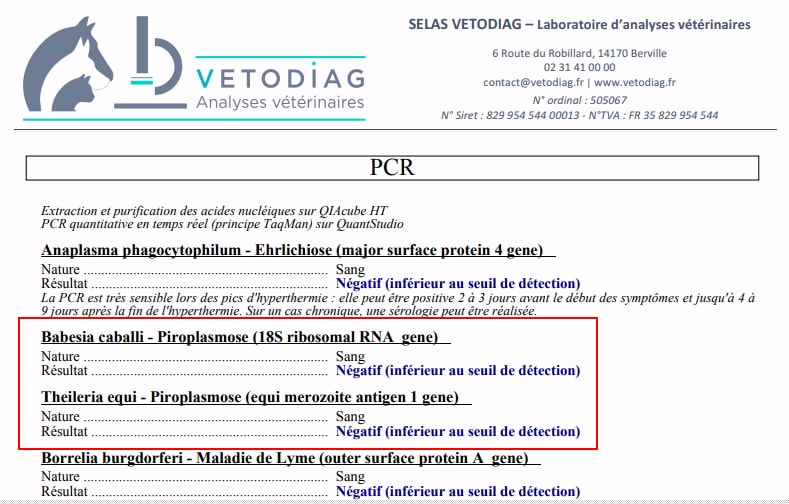
Above left: blood smears showing B. caballi and T. equi on red blood cells. Above right: PCR results for B. caballi and T. equi (negative in this case).
Click on the images to enlarge them.
Click on the images to enlarge them.
Microscopy - blood smear
During the acute phase a blood smear (initially thin, but thick may increase sensitivity if examined by someone experienced) should be made from superficial capillary blood (e.g. from the ear) and examined under the microscope for the presence of the parasites. Seeing (and accurately identifying) the parasites is diagnostic for piroplasmosis (see image above left), but not seeing the parasites does not rule out piroplasmosis as the level of parasites is low even in the acute phase* (particularly for B. caballi infections). Microscopy is unlikely to be useful for chronic cases.
*T. equi usually infects 1-7% of RBCs in horses showing signs of clinical disease, but may infect >20% (and up to 95%).
B. caballi rarely infects more than 1% of RBCs and may infect <0.1%.
PCR/Serology
Blood will be sent off to a laboratory for PCR and/or serology testing. Laboratories in France that test for piroplasmosis include Frank Duncombe and Vetodiag.
PCR (polymerase chain reaction) looks for and confirms the presence of parasite DNA and is considered highly specific and sensitive. PCR can detect low levels of parasitic infection and is best for chronic infections.
Serology measures the horse's immune response (the presence of antibodies) to the parasitic infection, and can detect carriers without symptoms as well as clinical infections, but cannot distinguish between whether the horse is currently infected or has been infected. Horses infected with T. equi produce antibodies against merozoites within 7 to 11 days, with levels peaking at 30 to 45 days. Horses infected with B. caballi also produce antibodies but less is known about this response. Serological tests include IFAT, ELISA and Western blot. None of these tests are perfect - a highly positive result is likely to be positive (although false positives are possible) but a negative result may not rule out infection - and ideally at least 2 different tests should be done.
Treatment
Treatment is the antiprotozoal drug Imidocarb, which is called Carbesia in France, given by intramuscular injection. In countries where equine piroplasmosis is endemic, treatment is usually aimed at eliminating clinical signs of the disease without eliminating the parasite from the body, as immunity depends on continued low level presence of the parasite, but where infected horses have been brought into a piroplasmosis-free country, the aim of treatment will be parasite elimination. T. equi is more difficult to treat than B. caballi. Recommended treatment for elimination of the parasites suggests 2 doses of 2.2 mg/kg 24 hours apart for B. caballi, and 4 doses of 4 mg/kg 72 hours apart for T. equi - treatment is likely to be less than this in countries where EP is endemic (e.g. France).
Imidocarb/Carbesia is an anticholinesterase and treated horses should be monitored for associated side effects such as colic, diarrhoea, increased salivation, sweating, heavy breathing, agitation and recumbency, and the vet will usually give injections of NSAIDs (anti-inflammatory pain relief) e.g. Nefotek (ketoprofen) and/or anti-spasmodic e.g. Buscopan, at the same time. Side effects are usually seen immediately after Imidocarb has been given and are rarely life-threatening. Swelling and muscle inflammation around the injection site are common, and injection sites should be rotated and monitored. Imidocarb is cleared by the liver and kidneys and at high doses toxicity can damage these organs. Note that donkeys and mules are particularly sensitive to Imidocarb and should not receive the higher dose.
Treatment should include supportive care for clinical signs as appropriate, and could involve anti-inflammatory medication (NSAIDS), pain relief, fluid treatment (e.g. intravenous fluid) for dehydrated horses/horses with kidney damage, and rarely, blood transfusion for cases with severe anaemia.
Management and Diet
Management includes appropriate nursing, rest and a good diet that provides recommended levels of energy, protein, minerals, vitamins and essential fatty acids - but not increased iron. Vets sometimes suggest an iron or "blood building" supplement (e.g. Red Cell) for horses with piroplasmosis. Such supplements usually contain large amounts of iron and are not recommended for horses with hemolytic anaemia (or any form of anaemia other than possibly severe haemorrhage and blood loss). With hemolytic anaemia, red blood cells are broken down in the body, releasing iron, which is locked away by the body until it is recycled into new red blood cells. Iron is toxic and difficult to get rid of from the body. Besides, the horse's natural forage diet is high in iron. See Anaemia and Iron Supplements.
Supporting immunity and new RBC development is important, and specifically the diet should include quality protein, e.g. micronized whole soya beans or whey protein/whey protein isolate, and provide at least 100% and probably 150-200% of the RDA for copper (important for RBC building and almost always deficient in a forage diet), the RDA being 100 mg for a 500 kg horse, so 150 to 200 mg/day copper - a horse eating 2% bodyweight in grass or hay is likely to ingest 40 to 60 mg of copper, leaving 90 to 160 mg copper to be supplied in bucket feed. Copper should be balanced by zinc in a 1 copper to 4 zinc ratio, so if providing 150 mg copper in the total diet, provide 600 mg zinc in the total diet. Plus 1 to 1.5 mg selenium in the total diet. If the horse is not eating well, give appetizing, easy to digest feed, ideally based on rapidly fermentable fibre such as sugar beet to provide slow release energy and to carry minerals and protein. Try to avoid making significant changes to the diet.
Immunity
Acute disease is uncommon in areas where piroplasmosis is endemic. Once a horse has been infected with either B. caballi or T. equi, it develops immunity against that form of disease, and (if not treated until elimination of the parasites) becomes a carrier. Without treatment, horses infected with B. caballi may completely eliminate it from their blood after around 3 to 5 years, but horses infected with T. equi remain life-long carriers. If brood mares are infected, foals can be infected in the womb and be healthy carriers. New born foals may be exposed to the parasites while still protected by maternal antibodies.
To prevent / help identify piroplasmosis
Websites with information about equine piroplasmosis
Int J Environ Res Public Health. 2019 May; 16(10): 1736. doi: 10.3390/ijerph16101736
A Review on Equine Piroplasmosis: Epidemiology, Vector Ecology, Risk Factors, Host Immunity, Diagnosis and Control
Onyiche et al.
Equine Piroplasmosis - OIE Terrestrial Manual 2018
Equine Piroplasmosis - Anna Spickler, 2018
FAQ Regarding Equine Piroplasmosis (EP) - AAEP
Equine piroplasmosis: What, how and why - Ed Kane 2016 - DVM360
Adam MI, Pikalo J, Snyder A, Steinrigl A, Koeller G, Schusser GF
Equine Piroplasmosis – a case of severe Babesia caballi infection associated with acute renal failure
Berliner und Münchener tierärztliche Wochenschrift Nov 2016 130:113 - 118. DOI: 10.2376/0005-9366-16064
(full pdf available online)
Osman SA
Clinical, haematological and therapeutic studies on babesiosis in Arabian horses in the Qassim region, central of Saudi Arabia
Journal of Applied Animal Research 2017, 45:1, 118-121, DOI: 10.1080/09712119.2015.1124339
Scoles GA, Ueti MW
Vector Ecology of Equine Piroplasmosis
Annual Review of Entomology Jan 2015 Vol 60: 561-580 https://doi.org/10.1146/annurev-ento-010814-021110
Wise LN, Pelzel-McCluskey AM, Mealey RH, Knowles DP
Equine Piroplasmosis
Vet Clin North Am Equine Pract. 2014 Dec;30(3):677-93. doi: 10.1016/j.cveq.2014.08.008 (DeepDyve)
J Vet Intern Med 2013;27:1334–1346
Review of Equine Piroplasmosis
L.N. Wise, L.S. Kappmeyer, R.H. Mealey, and D.P. Knowles
Equine Piroplasmosis - USDA APHIS 2020
APHIS Factsheet: Equine Piroplasmosis - USDA APHIS 2009
A Literature Review of Equine Piroplasmosis - USDA APHIS 2010
Traub-Dargatz JL, Short MA, Pelzel AM,Norman TE, Knowles DP
Equine Piroplasmosis
AAEP Proceedings Vol 56 2010
Equine Piroplasmosis - OIE World Animal Health 2009
Equine Piroplasmosis in Equine Infectious Diseases - edited by Debra C. Sellon, Maureen T. Long 2007
About Equine Piroplasmosis - Veterinary Diagnostic Services, University of Glasgow
Information in French
Piroplasmoses - RESPE
Carbesia (Imidocarb) RCP (datasheet)
La piroplasmose chez le cheval : une maladie parasitaire du système sanguin - www.classequine.com
During the acute phase a blood smear (initially thin, but thick may increase sensitivity if examined by someone experienced) should be made from superficial capillary blood (e.g. from the ear) and examined under the microscope for the presence of the parasites. Seeing (and accurately identifying) the parasites is diagnostic for piroplasmosis (see image above left), but not seeing the parasites does not rule out piroplasmosis as the level of parasites is low even in the acute phase* (particularly for B. caballi infections). Microscopy is unlikely to be useful for chronic cases.
*T. equi usually infects 1-7% of RBCs in horses showing signs of clinical disease, but may infect >20% (and up to 95%).
B. caballi rarely infects more than 1% of RBCs and may infect <0.1%.
PCR/Serology
Blood will be sent off to a laboratory for PCR and/or serology testing. Laboratories in France that test for piroplasmosis include Frank Duncombe and Vetodiag.
PCR (polymerase chain reaction) looks for and confirms the presence of parasite DNA and is considered highly specific and sensitive. PCR can detect low levels of parasitic infection and is best for chronic infections.
Serology measures the horse's immune response (the presence of antibodies) to the parasitic infection, and can detect carriers without symptoms as well as clinical infections, but cannot distinguish between whether the horse is currently infected or has been infected. Horses infected with T. equi produce antibodies against merozoites within 7 to 11 days, with levels peaking at 30 to 45 days. Horses infected with B. caballi also produce antibodies but less is known about this response. Serological tests include IFAT, ELISA and Western blot. None of these tests are perfect - a highly positive result is likely to be positive (although false positives are possible) but a negative result may not rule out infection - and ideally at least 2 different tests should be done.
Treatment
Treatment is the antiprotozoal drug Imidocarb, which is called Carbesia in France, given by intramuscular injection. In countries where equine piroplasmosis is endemic, treatment is usually aimed at eliminating clinical signs of the disease without eliminating the parasite from the body, as immunity depends on continued low level presence of the parasite, but where infected horses have been brought into a piroplasmosis-free country, the aim of treatment will be parasite elimination. T. equi is more difficult to treat than B. caballi. Recommended treatment for elimination of the parasites suggests 2 doses of 2.2 mg/kg 24 hours apart for B. caballi, and 4 doses of 4 mg/kg 72 hours apart for T. equi - treatment is likely to be less than this in countries where EP is endemic (e.g. France).
Imidocarb/Carbesia is an anticholinesterase and treated horses should be monitored for associated side effects such as colic, diarrhoea, increased salivation, sweating, heavy breathing, agitation and recumbency, and the vet will usually give injections of NSAIDs (anti-inflammatory pain relief) e.g. Nefotek (ketoprofen) and/or anti-spasmodic e.g. Buscopan, at the same time. Side effects are usually seen immediately after Imidocarb has been given and are rarely life-threatening. Swelling and muscle inflammation around the injection site are common, and injection sites should be rotated and monitored. Imidocarb is cleared by the liver and kidneys and at high doses toxicity can damage these organs. Note that donkeys and mules are particularly sensitive to Imidocarb and should not receive the higher dose.
Treatment should include supportive care for clinical signs as appropriate, and could involve anti-inflammatory medication (NSAIDS), pain relief, fluid treatment (e.g. intravenous fluid) for dehydrated horses/horses with kidney damage, and rarely, blood transfusion for cases with severe anaemia.
Management and Diet
Management includes appropriate nursing, rest and a good diet that provides recommended levels of energy, protein, minerals, vitamins and essential fatty acids - but not increased iron. Vets sometimes suggest an iron or "blood building" supplement (e.g. Red Cell) for horses with piroplasmosis. Such supplements usually contain large amounts of iron and are not recommended for horses with hemolytic anaemia (or any form of anaemia other than possibly severe haemorrhage and blood loss). With hemolytic anaemia, red blood cells are broken down in the body, releasing iron, which is locked away by the body until it is recycled into new red blood cells. Iron is toxic and difficult to get rid of from the body. Besides, the horse's natural forage diet is high in iron. See Anaemia and Iron Supplements.
Supporting immunity and new RBC development is important, and specifically the diet should include quality protein, e.g. micronized whole soya beans or whey protein/whey protein isolate, and provide at least 100% and probably 150-200% of the RDA for copper (important for RBC building and almost always deficient in a forage diet), the RDA being 100 mg for a 500 kg horse, so 150 to 200 mg/day copper - a horse eating 2% bodyweight in grass or hay is likely to ingest 40 to 60 mg of copper, leaving 90 to 160 mg copper to be supplied in bucket feed. Copper should be balanced by zinc in a 1 copper to 4 zinc ratio, so if providing 150 mg copper in the total diet, provide 600 mg zinc in the total diet. Plus 1 to 1.5 mg selenium in the total diet. If the horse is not eating well, give appetizing, easy to digest feed, ideally based on rapidly fermentable fibre such as sugar beet to provide slow release energy and to carry minerals and protein. Try to avoid making significant changes to the diet.
Immunity
Acute disease is uncommon in areas where piroplasmosis is endemic. Once a horse has been infected with either B. caballi or T. equi, it develops immunity against that form of disease, and (if not treated until elimination of the parasites) becomes a carrier. Without treatment, horses infected with B. caballi may completely eliminate it from their blood after around 3 to 5 years, but horses infected with T. equi remain life-long carriers. If brood mares are infected, foals can be infected in the womb and be healthy carriers. New born foals may be exposed to the parasites while still protected by maternal antibodies.
To prevent / help identify piroplasmosis
- There is no vaccine for equine piroplasmosis.
- Check for ticks every day, particularly: around and inside the ears, under the forelock and mane, under the jaw, around the girth & between the front legs, and all down the legs, particularly the back of the fetlock and pastern, around the top of the hind legs/thighs and sheath/udder area, right down the hind legs, particulary the back of the fetlock and pastern, and the length of the dock. Ticks like thin skin and often hide under hair and in crevices.
- Remove ticks if found, being careful not to leave any part of the tick in the horse - a Tire-Tique which uses a twisting action is good for removing ticks whole. Not removing a tick correctly can stimulate the tick to secrete more saliva, cause regurgitation, introduce other tick-body secretions or excretions into the wound, or increase the risk of secondary infection around the bite. After removing a tick wash the area and/or apply antiseptic
- Treat horses with an insect repellent that deters ticks, usually with the active ingredient pyrethrin or pyrethroid, e.g. diluted Butox (active ingredient deltramethrin, a pyrethroid).
- Ticks climb to the tips of grasses and shrubs (but not trees) to wait for host animals to brush by, then crawl onto the host, so try to keep horses away from long grass, plants and bushes. Top/mow fields and cut back borders (but without harming wildlife like hedgehogs!) and check horses carefully after hacking through long grass/plants.
- Risk increases with immunological naivety (i.e. horses that haven't previously been exposed to EP) and with increased density of infected ticks and infected horses. Horses suffering from stress, a low immune response or with their spleen removed may be more susceptible to/at greater risk from EP. Carriers have had relapses associated with stress, strenuous exercise, immunosuppression and steroid administration.
- Check your horse's temperature, heart rate and respiration rate at the first sign he/she may not be quite right.
- Watch your horse urinating and check the urine is light creamy/yellowy, not red or brown (however this is not an early sign of piroplasmosis and not always seen).
Websites with information about equine piroplasmosis
Int J Environ Res Public Health. 2019 May; 16(10): 1736. doi: 10.3390/ijerph16101736
A Review on Equine Piroplasmosis: Epidemiology, Vector Ecology, Risk Factors, Host Immunity, Diagnosis and Control
Onyiche et al.
Equine Piroplasmosis - OIE Terrestrial Manual 2018
Equine Piroplasmosis - Anna Spickler, 2018
FAQ Regarding Equine Piroplasmosis (EP) - AAEP
Equine piroplasmosis: What, how and why - Ed Kane 2016 - DVM360
Adam MI, Pikalo J, Snyder A, Steinrigl A, Koeller G, Schusser GF
Equine Piroplasmosis – a case of severe Babesia caballi infection associated with acute renal failure
Berliner und Münchener tierärztliche Wochenschrift Nov 2016 130:113 - 118. DOI: 10.2376/0005-9366-16064
(full pdf available online)
Osman SA
Clinical, haematological and therapeutic studies on babesiosis in Arabian horses in the Qassim region, central of Saudi Arabia
Journal of Applied Animal Research 2017, 45:1, 118-121, DOI: 10.1080/09712119.2015.1124339
Scoles GA, Ueti MW
Vector Ecology of Equine Piroplasmosis
Annual Review of Entomology Jan 2015 Vol 60: 561-580 https://doi.org/10.1146/annurev-ento-010814-021110
Wise LN, Pelzel-McCluskey AM, Mealey RH, Knowles DP
Equine Piroplasmosis
Vet Clin North Am Equine Pract. 2014 Dec;30(3):677-93. doi: 10.1016/j.cveq.2014.08.008 (DeepDyve)
J Vet Intern Med 2013;27:1334–1346
Review of Equine Piroplasmosis
L.N. Wise, L.S. Kappmeyer, R.H. Mealey, and D.P. Knowles
Equine Piroplasmosis - USDA APHIS 2020
APHIS Factsheet: Equine Piroplasmosis - USDA APHIS 2009
A Literature Review of Equine Piroplasmosis - USDA APHIS 2010
Traub-Dargatz JL, Short MA, Pelzel AM,Norman TE, Knowles DP
Equine Piroplasmosis
AAEP Proceedings Vol 56 2010
Equine Piroplasmosis - OIE World Animal Health 2009
Equine Piroplasmosis in Equine Infectious Diseases - edited by Debra C. Sellon, Maureen T. Long 2007
About Equine Piroplasmosis - Veterinary Diagnostic Services, University of Glasgow
Information in French
Piroplasmoses - RESPE
Carbesia (Imidocarb) RCP (datasheet)
La piroplasmose chez le cheval : une maladie parasitaire du système sanguin - www.classequine.com
Cases of Equine Piroplasmosis
Scoles GA, Hutcheson HJ, Schlater JL, Hennager SG, Pelzel AM, Knowles DP
Equine Piroplasmosis Associated with Amblyomma cajennense Ticks, Texas, USA
EID Oct 2011 Vol 17, No. 10
In October 2009 1 mare in Texas showed clinical signs of equine piroplasmosis and was found positive for T. equi by ELISA. 359 horses on the ranch were tested by ELISA, 292 (81%) were seropositive for T. equi. Ticks were found on 228 horses.
104 ticks (taken from horses that were 93% positive for T. equi) were placed on an uninfected horse 30 October. That horse had a fever (>39'C) 14 days after tick introduction, but no other clinical signs. Sighting of parasitized RBCs on blood slide peaked at 0.3% on day 17. Serology and PCR confirmed T. equi infection.
29 ticks (taken from horses that were at least 64% positive for T. equi) were placed on a second uninfected horse 30 October. That horse had a slight fever (39'C) 15 days after tick introduction, but no other clinical signs. Parasites were not seen on blood slides. PCR was positive for T. equi 42 days, and ELISA 87 days after tick introduction.
This research showed that T. equi can be transmitted interstadially, i.e. by a tick feeding on an infected horse and then infecting another horse, without going through a developmental change (however, the ticks were removed from the infected horses, they didn't drop off naturally). Note that raised temperature was the only clinical sign seen in both the intentionally infected horses.
Scoles GA, Hutcheson HJ, Schlater JL, Hennager SG, Pelzel AM, Knowles DP
Equine Piroplasmosis Associated with Amblyomma cajennense Ticks, Texas, USA
EID Oct 2011 Vol 17, No. 10
In October 2009 1 mare in Texas showed clinical signs of equine piroplasmosis and was found positive for T. equi by ELISA. 359 horses on the ranch were tested by ELISA, 292 (81%) were seropositive for T. equi. Ticks were found on 228 horses.
104 ticks (taken from horses that were 93% positive for T. equi) were placed on an uninfected horse 30 October. That horse had a fever (>39'C) 14 days after tick introduction, but no other clinical signs. Sighting of parasitized RBCs on blood slide peaked at 0.3% on day 17. Serology and PCR confirmed T. equi infection.
29 ticks (taken from horses that were at least 64% positive for T. equi) were placed on a second uninfected horse 30 October. That horse had a slight fever (39'C) 15 days after tick introduction, but no other clinical signs. Parasites were not seen on blood slides. PCR was positive for T. equi 42 days, and ELISA 87 days after tick introduction.
This research showed that T. equi can be transmitted interstadially, i.e. by a tick feeding on an infected horse and then infecting another horse, without going through a developmental change (however, the ticks were removed from the infected horses, they didn't drop off naturally). Note that raised temperature was the only clinical sign seen in both the intentionally infected horses.
Colic
Colic simply means abdominal pain - it usually suggests a problem in the digestive tract, but can involve other organs in the abdomen. The good news is that around 90% of colics respond to medical treatment (antispasmodics and pain relief) or resolve on their own, but around 10% of cases are very serious and need surgery, and the sooner this is recognised and performed, the better the outcome is likely to be.
Signs of colic include:
Change in behaviour
Restlessness
Pawing at the ground
Refusing food
Sweating
Increased heart rate and respiration rate
Kicking at the stomach
Looking round at the abdomen
Stretching out as if to urinate
Rolling or trying to roll, or lying down unusually
Change in mucous membrane colour - gums should be pale pink, any change in colour towards red or purple may indicate endotoxaemia and dehydration associated with a severe colic.
To reduce the risk of and help prevent colic:
Make all changes to feed as gradually as possible. Even changing to new but similar hay should be done over 2 to 3 weeks if possible. Feeds can be removed abruptly from the diet, but should never be added in large quantities abruptly, as any change in the diet will cause the gut microbiome to change.
Keep concentrate bucket feeds small, and keep the amount of starch in a feed as small as possible. Apart from intensely working horses, many horses do well on a fibre diet with a balancer to ensure adequate protein, minerals and vitamins.
Do not feed anything with dubious hygienic quality - NEVER risk feeding anything with signs of mould or feed that has been damaged in any way (e.g. become wet). Horses are very susceptible to mycotoxins and moulds in feed. Discard any feed that could contain hazards such as plastic, string, needles.
Feed at least 1.5% of a horse's ideal bodyweight in forage. Although straw can be fed, many experts recommend that straw should make up no more than 25% of the diet, teeth must be functioning well and straw must be introduced very gradually, to reduce the risk of impaction colic.
Ensure clean water is always available. In cold weather, offer moist feeds and warm water. Not drinking enough in cold weather is a high risk for impaction colic.
Ensure teeth are functioning well - have adult horses checked by a qualified EDT or specialist vet at least every year, youngsters and aged horses every 6 months.
Ensure worm burdens are not significantly high - although now recommendations are not to remove all worms, worm egg count frequently to ensure worm burdens stay within acceptable ranges. A saliva test is available for tapeworms, but currently (2021) there is still no test for encysted small redworms, so worming once a year (between November and February) with Equest (moxidectin) may be sensible.
Monitor horses closely after stress or change, e.g. hard exercise if not sufficiently conditioned or after eating, travelling, change of routine or environment, loss of a companion, any change to exercise or diet. Impaction colic is often seen when horses are put on box rest.
Movement helps gut motility - try to give regular exercise and turnout.
Avoid grazing on sandy soils. If horses live on sandy soil, try to avoid short grass, feed plenty of forage (hay may be as good as psyllium for clearing sand from the gut), do not feed directly from the ground, use psyllium regularly to help remove sand from the gut.
Never allow horses to eat mown grass cuttings, or anything that has fermented. Do not soak hay or sugar beet for long in hot weather, feed soon after soaking and remove uneaten food before it can ferment.
Know your horse's usual heart rate, respiration rate, temperature, capillary refill time, mucous membrane colour and feel (how slippery the gums are).
What to do if your horse has colic
Phone the vet - colic should always be treated as an emergency.
Ideally check heart rate, respiration rate, temperature, mouth mucous membrane colour (normal membranes are pale pink and moist) and feel and report these and the clinical signs you are seeing to your vet - this helps them to know how quickly they must get to you and to recommend anything you can do in the meantime.
Remove feed and hay from the horse (and water until a vet says it is ok to allow access to water).
Put the horse in a safe area.
Do not stop the horse from rolling. Keep yourself safe.
If signs are not too severe, walking a horse may help clear gas, but check with your vet first, and do not walk a horse to exhaustion.
What your vet might do
Your vet will try to identify the cause of the colic, which part of the gut is affected and whether there is part or complete obstruction of the gut. An examination will usually involve:
Treatment
If there are no indications that surgery is needed, the vet will usually give short acting pain relief and assess again in 2 hours. After re-examination at 2 hours, if there is no improvement, a vet may either give pain relief and re-assess after a further 2 hours, or refer for surgery. If no improvement after 4 hours, a horse may be referred for surgery, as even though it may not have a surgical colic, there may be a risk of endotoxaemia.
Increased severity of pain, degree of abdominal distention and frequency of gut sounds can be used to evaluate how serious the colic is. Moderate to severe colic signs, persistent colic that doesn't respond to medical treatment, and return of colic signs following pain relief are all associated with the need for surgery.
Horses should be given pain relief before traveling to a clinic.
Severe colic can lead to dehydration, hypovolemia and shock. Signs of moderate dehydration and hypovolemia: quiet but alert and responsive, heart rate 62-76 bpm, mucous membranes variable colour, sticky to dry, capillary refill >2 seconds, extremities start to become cooler, slow jugular refill and variable pulse quality. Signs of severe dehydration and shock: dull, heart rate >80 bpm, mucous membranes dry and red/purple or pale, capillar refill time >3 seconds, cool extremities, poor jugular refill, peripheral pulses difficult to feel.
Colic: prevention and management - Blue Cross
Colic types and causes - University of Liverpool Equine Hospital
Colic simply means abdominal pain - it usually suggests a problem in the digestive tract, but can involve other organs in the abdomen. The good news is that around 90% of colics respond to medical treatment (antispasmodics and pain relief) or resolve on their own, but around 10% of cases are very serious and need surgery, and the sooner this is recognised and performed, the better the outcome is likely to be.
Signs of colic include:
Change in behaviour
Restlessness
Pawing at the ground
Refusing food
Sweating
Increased heart rate and respiration rate
Kicking at the stomach
Looking round at the abdomen
Stretching out as if to urinate
Rolling or trying to roll, or lying down unusually
Change in mucous membrane colour - gums should be pale pink, any change in colour towards red or purple may indicate endotoxaemia and dehydration associated with a severe colic.
To reduce the risk of and help prevent colic:
Make all changes to feed as gradually as possible. Even changing to new but similar hay should be done over 2 to 3 weeks if possible. Feeds can be removed abruptly from the diet, but should never be added in large quantities abruptly, as any change in the diet will cause the gut microbiome to change.
Keep concentrate bucket feeds small, and keep the amount of starch in a feed as small as possible. Apart from intensely working horses, many horses do well on a fibre diet with a balancer to ensure adequate protein, minerals and vitamins.
Do not feed anything with dubious hygienic quality - NEVER risk feeding anything with signs of mould or feed that has been damaged in any way (e.g. become wet). Horses are very susceptible to mycotoxins and moulds in feed. Discard any feed that could contain hazards such as plastic, string, needles.
Feed at least 1.5% of a horse's ideal bodyweight in forage. Although straw can be fed, many experts recommend that straw should make up no more than 25% of the diet, teeth must be functioning well and straw must be introduced very gradually, to reduce the risk of impaction colic.
Ensure clean water is always available. In cold weather, offer moist feeds and warm water. Not drinking enough in cold weather is a high risk for impaction colic.
Ensure teeth are functioning well - have adult horses checked by a qualified EDT or specialist vet at least every year, youngsters and aged horses every 6 months.
Ensure worm burdens are not significantly high - although now recommendations are not to remove all worms, worm egg count frequently to ensure worm burdens stay within acceptable ranges. A saliva test is available for tapeworms, but currently (2021) there is still no test for encysted small redworms, so worming once a year (between November and February) with Equest (moxidectin) may be sensible.
Monitor horses closely after stress or change, e.g. hard exercise if not sufficiently conditioned or after eating, travelling, change of routine or environment, loss of a companion, any change to exercise or diet. Impaction colic is often seen when horses are put on box rest.
Movement helps gut motility - try to give regular exercise and turnout.
Avoid grazing on sandy soils. If horses live on sandy soil, try to avoid short grass, feed plenty of forage (hay may be as good as psyllium for clearing sand from the gut), do not feed directly from the ground, use psyllium regularly to help remove sand from the gut.
Never allow horses to eat mown grass cuttings, or anything that has fermented. Do not soak hay or sugar beet for long in hot weather, feed soon after soaking and remove uneaten food before it can ferment.
Know your horse's usual heart rate, respiration rate, temperature, capillary refill time, mucous membrane colour and feel (how slippery the gums are).
What to do if your horse has colic
Phone the vet - colic should always be treated as an emergency.
Ideally check heart rate, respiration rate, temperature, mouth mucous membrane colour (normal membranes are pale pink and moist) and feel and report these and the clinical signs you are seeing to your vet - this helps them to know how quickly they must get to you and to recommend anything you can do in the meantime.
Remove feed and hay from the horse (and water until a vet says it is ok to allow access to water).
Put the horse in a safe area.
Do not stop the horse from rolling. Keep yourself safe.
If signs are not too severe, walking a horse may help clear gas, but check with your vet first, and do not walk a horse to exhaustion.
What your vet might do
Your vet will try to identify the cause of the colic, which part of the gut is affected and whether there is part or complete obstruction of the gut. An examination will usually involve:
- physical examination & review of history - heart rate, respiration rate, temperature, capillary refill time, oral mucous membrane colour & moistness, is the horse alert or dull, what signs of pain is the horse showing (looking at the abdomen, pawing, lying down, rolling). NB a horse with a heart rate >60 bpm should have a naso-gastric tube inserted immediately as this can be a sign of pending fatal gastric rupture. If the heart rate is >70 bpm the horse is likely to have some degree of shock.
- listening to gut sounds - are they normal, more/less than normal, on one or both sides
- looking for distention of the abdomen (the horse should be standing square)
- considering when dung was last passed and whether there are faeces in the rectum
- naso-gastric reflux
- rectal exam - only the back 1/3 of the abdomen can be examined and often changes can only be detected when they become quite marked. Carries a risk of tearing the gut wall. The horse must be adequately restrained and sedated if necessary.
- ultrasound - may be used instead of (particularly in small breeds/foals) or as well as a rectal exam
- blood tests - PCV (to assess hydration), lactate, creatinine
- examining peritoneal fluid for colour and assaying red and white blood cells, lactate and protein
- gastroscopy
Treatment
If there are no indications that surgery is needed, the vet will usually give short acting pain relief and assess again in 2 hours. After re-examination at 2 hours, if there is no improvement, a vet may either give pain relief and re-assess after a further 2 hours, or refer for surgery. If no improvement after 4 hours, a horse may be referred for surgery, as even though it may not have a surgical colic, there may be a risk of endotoxaemia.
Increased severity of pain, degree of abdominal distention and frequency of gut sounds can be used to evaluate how serious the colic is. Moderate to severe colic signs, persistent colic that doesn't respond to medical treatment, and return of colic signs following pain relief are all associated with the need for surgery.
Horses should be given pain relief before traveling to a clinic.
Severe colic can lead to dehydration, hypovolemia and shock. Signs of moderate dehydration and hypovolemia: quiet but alert and responsive, heart rate 62-76 bpm, mucous membranes variable colour, sticky to dry, capillary refill >2 seconds, extremities start to become cooler, slow jugular refill and variable pulse quality. Signs of severe dehydration and shock: dull, heart rate >80 bpm, mucous membranes dry and red/purple or pale, capillar refill time >3 seconds, cool extremities, poor jugular refill, peripheral pulses difficult to feel.
Colic: prevention and management - Blue Cross
Colic types and causes - University of Liverpool Equine Hospital
Laminitis
|
When a horse gets laminitis, unless it is obviously ill with a raised temperature (Sepsis Related Laminitis) or has supporting limb laminitis following a severe and usually reasonably long-term non-weightbearing lameness in another limb, the laminitis will almost certainly be caused by Insulin Dysregulation (ID), and the horse will either have Equine Metabolic Syndrome alone, or plus PPID (formerly called Cushing's Disease).
Successful treatment of laminitis depends on identifying and removing/treating the cause (requiring endocrine blood testing) AND supporting and realigning the feet (requiring x-rays). |
|
Did you know?
|
Find out everything you need to know about laminitis, with information specific to France, at www.thelaminitissite.org, a website created and run by CHG member Andrea Jones
Atypical Myopathy (AM)
\June 2013: Atypical Myopathy - Liphook Equine Hospital client update
Atypical Myopathy (AM) is an acute and severe rhabdomyolysis that is not related to exercise, with a high mortality rate (~ 74%), and is found in Europe (UK, France, The Netherlands, Belgium, Germany have reported cases). Very little is known about the disease, but recent research has concluded that AM is caused by a toxin called hypoglycin A found in sycamore seeds (Acer pseudoplatanus) in Europe. In the USA the same toxin has been found in box elder tree seeds (Acer negundo) and causes Seasonal Pasture Myopathy (SPM). AM is known to involve a metabolic defect - multiple acyl-CoA dehydrogenase deficiency (MADD), which blocks fatty acid energy metabolism in the mitochondria, and muscle cells of severely affected horses can be completely depleted of carbohydrates. AM likely involves massive muscle destruction. Horses that die from AM generally do so very quickly, within 1 - 2 days of symptoms being seen, and in recent research all nonsurvivors died or were put down within 10 days of symptoms being seen. More..
Atypical Myopathy (AM) is an acute and severe rhabdomyolysis that is not related to exercise, with a high mortality rate (~ 74%), and is found in Europe (UK, France, The Netherlands, Belgium, Germany have reported cases). Very little is known about the disease, but recent research has concluded that AM is caused by a toxin called hypoglycin A found in sycamore seeds (Acer pseudoplatanus) in Europe. In the USA the same toxin has been found in box elder tree seeds (Acer negundo) and causes Seasonal Pasture Myopathy (SPM). AM is known to involve a metabolic defect - multiple acyl-CoA dehydrogenase deficiency (MADD), which blocks fatty acid energy metabolism in the mitochondria, and muscle cells of severely affected horses can be completely depleted of carbohydrates. AM likely involves massive muscle destruction. Horses that die from AM generally do so very quickly, within 1 - 2 days of symptoms being seen, and in recent research all nonsurvivors died or were put down within 10 days of symptoms being seen. More..
Leptospirosis
Leptospirosis is a widespread zoonotic (can be spread from animals to people) bacterial disease, caused by Leptospira species. It is readily transmitted between species usually directly or indirectly from contaminated urine (or other body fluids), particularly in stagnant or contaminated water, also soil and in feed/forage. The disease can enter through the mouth, eyes, nose or any broken skin. Leptospirosis can be carried by wild and domestic animals, particularly rodents - rats are common carriers, mice, voles, hedgehogs, coypu are all known to carry leptospirosis. Infection is common in the autumn in some countries - moderate temperature and moisture provide optimal conditions for transmission of the disease.
In horses infections are often sub-clinical (without symptoms) but can cause abortion and recurrent uveitis.
Clinical forms of the disease are also seen, with fever (raised temperature), anorexia, lethargy/listlessness/depression and jaundice being the commonly reported symptoms, and also weakness, respiratory distress, haematuria (blood in the urine), renal dysfunction, hepatic dysfunction, recurrent uveitis, abortion, stillbirth, prematurely born foals.
Leptospirosis may be a common cause of recurrent uveitis (mood blindness), which generally develops several months (one report said 2-8 months, another 12 - 24 months) after the initial infection.
The fever usually lasts 2- 3 days, bacteremia (bacteria in the blood) usually occurs 4 - 10 days after infection and may last from hours to days. The severity of the infection is likely to depend on the strain of leptospirosis and the immune status of the horse - it is often serious in foals but the prognosis is generally good in adult horses, other than for the risk of recurrent uveitis (is it likely to be more serious in older horses too if their immune system is weakened - perhaps not if they have some immunity?). It may be more severe if caught from a different species rather than from another horse.
Testing for leptospirosis is not straightforward and is carried out by specialist laboratories. Frank Duncombe Laboratory in Normandy tests for leptospirosis for horses in France.
During acute infection, leukocytosis and neutrophilia may be seen, perhaps also lymphopaenia, and hyperbilirubinemia is sometimes seen.
Treatment: Leptospirosis is treated with antibiotics - e.g. oxytetracycline, penicillin or streptomycin.
Prevention: do not allow horses to drink stagnant or any water that may be contaminated with urine, keep rodents away from feed stores, do not feed from the ground where rodents or wild animals may have urinated.
Equine Infectious Diseases ch 34 - Debra C Sellon, Maureen T Long 2007
Current Therapy in Equine Medicine 6 ch 33 - N Edward Robinson, Kim A Sprayberry 2009
Acta Veterinaria Scandinavica 2009, 51:15
Leptospira seroprevalence and associations between seropositivity, clinical disease and host factors in horsesV Båverud, A Gunnarsson, E Olsson Engvall, P Franzén and A Egenvall
Leptospirosis in Horses - The Merck Veterinary Manual
Equine leptospirosis (Proceedings)
Aug 1, 2008
Thomas Divers, DVM, DACVIM, DACVECC
African Journal of Microbiology Research Vol. 6(20), pp. 4384-4387, 30 May, 2012
Seroprevalence of leptospiral infection in horses, donkeys and mules in East Azerbaijan province
Hassanpour Ali and Safarmashaei Saeid
Preventive Veterinary Medicine Volume 13, Issue 2, June 1992, Pages 121–127
Factors for seropositivity to leptospirosis in horses
Y.G. Park, J.C. Gordon, S. Bech-Nielsen, R.D. Slemons
Horses admitted to hospital for various reasons were tested for leptospiral antibodies. Horses with eye conditions were most likely to be positive to leptospirosis, and horses admitted with laminitis and colic had a higher prevalence than horses with other conditions. (NB presumably this doesn't imply that leptospirosis causes laminitis and colic, it could be that horses kept at grass are more likely to get laminitis/colic and have more exposure to leptospirosis).
Vet Clin North Am Equine Pract. 1993 Aug;9(2):435-44
Leptospirosis
Bernard WV
Research into an equine vaccine against leptospirosis is to be carried out at Cornell:
Vaccine Against Equine Leptospirosis Dr. Yung-Fu Chang (2012)
European Journal of Epidemiology 17: 111-121, 2001
Role of the coypu (Myocastor coypus) in the epidemiology of leptospirosis in domestic animals and humans in France
V Michel, N Ruvoen-Clouet, A Menard, C Sonrier, C Fillonneau, F Rakotovao, J P Ganiere, G Andre-Fontaine
In horses infections are often sub-clinical (without symptoms) but can cause abortion and recurrent uveitis.
Clinical forms of the disease are also seen, with fever (raised temperature), anorexia, lethargy/listlessness/depression and jaundice being the commonly reported symptoms, and also weakness, respiratory distress, haematuria (blood in the urine), renal dysfunction, hepatic dysfunction, recurrent uveitis, abortion, stillbirth, prematurely born foals.
Leptospirosis may be a common cause of recurrent uveitis (mood blindness), which generally develops several months (one report said 2-8 months, another 12 - 24 months) after the initial infection.
The fever usually lasts 2- 3 days, bacteremia (bacteria in the blood) usually occurs 4 - 10 days after infection and may last from hours to days. The severity of the infection is likely to depend on the strain of leptospirosis and the immune status of the horse - it is often serious in foals but the prognosis is generally good in adult horses, other than for the risk of recurrent uveitis (is it likely to be more serious in older horses too if their immune system is weakened - perhaps not if they have some immunity?). It may be more severe if caught from a different species rather than from another horse.
Testing for leptospirosis is not straightforward and is carried out by specialist laboratories. Frank Duncombe Laboratory in Normandy tests for leptospirosis for horses in France.
During acute infection, leukocytosis and neutrophilia may be seen, perhaps also lymphopaenia, and hyperbilirubinemia is sometimes seen.
Treatment: Leptospirosis is treated with antibiotics - e.g. oxytetracycline, penicillin or streptomycin.
Prevention: do not allow horses to drink stagnant or any water that may be contaminated with urine, keep rodents away from feed stores, do not feed from the ground where rodents or wild animals may have urinated.
Equine Infectious Diseases ch 34 - Debra C Sellon, Maureen T Long 2007
Current Therapy in Equine Medicine 6 ch 33 - N Edward Robinson, Kim A Sprayberry 2009
Acta Veterinaria Scandinavica 2009, 51:15
Leptospira seroprevalence and associations between seropositivity, clinical disease and host factors in horsesV Båverud, A Gunnarsson, E Olsson Engvall, P Franzén and A Egenvall
Leptospirosis in Horses - The Merck Veterinary Manual
Equine leptospirosis (Proceedings)
Aug 1, 2008
Thomas Divers, DVM, DACVIM, DACVECC
African Journal of Microbiology Research Vol. 6(20), pp. 4384-4387, 30 May, 2012
Seroprevalence of leptospiral infection in horses, donkeys and mules in East Azerbaijan province
Hassanpour Ali and Safarmashaei Saeid
Preventive Veterinary Medicine Volume 13, Issue 2, June 1992, Pages 121–127
Factors for seropositivity to leptospirosis in horses
Y.G. Park, J.C. Gordon, S. Bech-Nielsen, R.D. Slemons
Horses admitted to hospital for various reasons were tested for leptospiral antibodies. Horses with eye conditions were most likely to be positive to leptospirosis, and horses admitted with laminitis and colic had a higher prevalence than horses with other conditions. (NB presumably this doesn't imply that leptospirosis causes laminitis and colic, it could be that horses kept at grass are more likely to get laminitis/colic and have more exposure to leptospirosis).
Vet Clin North Am Equine Pract. 1993 Aug;9(2):435-44
Leptospirosis
Bernard WV
Research into an equine vaccine against leptospirosis is to be carried out at Cornell:
Vaccine Against Equine Leptospirosis Dr. Yung-Fu Chang (2012)
European Journal of Epidemiology 17: 111-121, 2001
Role of the coypu (Myocastor coypus) in the epidemiology of leptospirosis in domestic animals and humans in France
V Michel, N Ruvoen-Clouet, A Menard, C Sonrier, C Fillonneau, F Rakotovao, J P Ganiere, G Andre-Fontaine
Euthanasia and body disposal in France
Euthanasia
"Euthanasia must be swift and free from pain and panic."
We understand that the only option for euthanasia in France is lethal injection. The drug of choice for euthanasia is Sodium Pentobarbital - Pentobarbital sodique in French - a barbiturate, (or a Pentobarbital combination). The drug T-61 is commonly used in France but is illegal in the UK and USA and considered inhumane - see below.
We recommend that you plan your horse's final moments well ahead of time, and check that your vet will use Sodium Pentobarbital.
For full details of euthanasia methods, see the AVMA Guidelines on Euthanasia June 2007
Page 11 for information about sodium pentobarbital/barbiturates and page 18 for information specific to horses.
Vets for Equine Welfare - Equine Euthanasia
"ACCEPTABLE METHODS OF EQUINE EUTHANASIA (preferred method)
Pentobarbital or a Pentobarbital Combination: This is the best choice for equine euthanasia. Because a large volume of solution must be injected, use of an intravenous catheter placed in the jugular vein will facilitate the procedure. In order to facilitate catheterization and minimize equine anxiety and stress, a tranquilizer such as acepromazine, or an alpha-2 adrenergic agonist should be administered."
Equine Protection Network - Euthanasia of Horses
"Sodium Pentobarbital
The barbiturate, Sodium Pentobarbital is the most widely used drug, and is the drug of choice for euthanizing horses. Barbiturates depress the central nervous system, with unconsciousness progressing to depression of breathing and finally cardiac arrest. The advantage of barbiturates is speed of action. This effect depends on the dose, concentration, and rate of injection. Barbiturates induce euthanasia smoothly, with minimal discomfort to the animal.
T-61
The drug T-61 is considered inhumane by many veterinarians. The horse is paralyzed but fully conscious. The horse is suffocating and is fully aware. This drug was often used to benefit the observers of a horse being euthanized, such as at the racetrack. Due to the horse's lack of movement the fans wrongly assumed that the horse was instantly dead. T-61 is a nonbarbiturate, non-narcotic mixture of three drugs. These drugs provide a combination of general anesthetic, curariform, and local anesthetic actions. T-61 has been withdrawn from the market and is no longer manufactured or commercially available in the United States. It is available in Canada. It contains a local anesthetic, a strong hypnotic agent that depresses the central nervous system causing unconsciousness and another drug which has a paralytic effect on the respiratory center and a relaxing effect on skeletal muscles."
Articles about euthanasia:
A Thoughtful Goodbye - Nikki James - www.flyingchanges.com
Euthanasia - How it's done - Habitat for Horses
"If horses don't go to Heaven, then Heaven's no place for me."" We always let the other horses come see the body. They need to do this, to understand what happened. The one time we didn't the horse's mate wandered the pasture for days hunting for her, neighing for hours on end. Let them know what happened. Horses understand more than we give them credit for. They need that few minutes with the body."
Body Disposal
It is illegal in France to bury an animal that weighs more than 40 kg - according to Le Code Rural Article L226-4
Les propriétaires ou détenteurs d’un cadavre d’animal ou d’un lot de cadavres d’animaux pesant au total plus de quarante kilogrammes sont tenus d’avertir dans les plus brefs délais la personne chargée de l’exécution du service public de l’équarrissage d’avoir à procéder à l’enlèvement du ou des cadavres.
Il est interdit par la loi d’enfouir, de jeter en quelque lieu que ce soit ou d’incinérer les cadavres d’animaux ou lots de cadavres d’animaux pesant au total plus de quarante kilogrammes.
Les Haras nationaux - Equarrissage
L'équarrissage, c'est quoi ?
Horses can be cremated following an autopsy at the Laboratoire Départemental d’Analyses et de Recherche de la Haute-Vienne in Limoges. You have to make arrangements to get the body there, at the lab there is equipment to move the body. Reports are that staff are very sensitive, cost for a 500 kg horse in December 2012 was just under 1000 euros for autopsy, private cremation and return of ashes.
According to ANIE, since October 2009 horses can be cremated in France without an autopsy:
Association Nationale pour l'Incinération des Equidés
www.incineris.fr
SERVICE D’INCINÉRATION pour les équidés have 2 centres where equine cremations can be carried out:
Vimoutiers dans l’Orne, Rue des Sorbiers - 61120 Vimoutiers Tél : 02 33 39 80 52
Château-Gaillard dans l’Ain, 255 rue Charles de Gaulle - 01500 Château-Gaillard Tél : 04 74 38 72 22
"Euthanasia must be swift and free from pain and panic."
We understand that the only option for euthanasia in France is lethal injection. The drug of choice for euthanasia is Sodium Pentobarbital - Pentobarbital sodique in French - a barbiturate, (or a Pentobarbital combination). The drug T-61 is commonly used in France but is illegal in the UK and USA and considered inhumane - see below.
We recommend that you plan your horse's final moments well ahead of time, and check that your vet will use Sodium Pentobarbital.
For full details of euthanasia methods, see the AVMA Guidelines on Euthanasia June 2007
Page 11 for information about sodium pentobarbital/barbiturates and page 18 for information specific to horses.
Vets for Equine Welfare - Equine Euthanasia
"ACCEPTABLE METHODS OF EQUINE EUTHANASIA (preferred method)
Pentobarbital or a Pentobarbital Combination: This is the best choice for equine euthanasia. Because a large volume of solution must be injected, use of an intravenous catheter placed in the jugular vein will facilitate the procedure. In order to facilitate catheterization and minimize equine anxiety and stress, a tranquilizer such as acepromazine, or an alpha-2 adrenergic agonist should be administered."
Equine Protection Network - Euthanasia of Horses
"Sodium Pentobarbital
The barbiturate, Sodium Pentobarbital is the most widely used drug, and is the drug of choice for euthanizing horses. Barbiturates depress the central nervous system, with unconsciousness progressing to depression of breathing and finally cardiac arrest. The advantage of barbiturates is speed of action. This effect depends on the dose, concentration, and rate of injection. Barbiturates induce euthanasia smoothly, with minimal discomfort to the animal.
T-61
The drug T-61 is considered inhumane by many veterinarians. The horse is paralyzed but fully conscious. The horse is suffocating and is fully aware. This drug was often used to benefit the observers of a horse being euthanized, such as at the racetrack. Due to the horse's lack of movement the fans wrongly assumed that the horse was instantly dead. T-61 is a nonbarbiturate, non-narcotic mixture of three drugs. These drugs provide a combination of general anesthetic, curariform, and local anesthetic actions. T-61 has been withdrawn from the market and is no longer manufactured or commercially available in the United States. It is available in Canada. It contains a local anesthetic, a strong hypnotic agent that depresses the central nervous system causing unconsciousness and another drug which has a paralytic effect on the respiratory center and a relaxing effect on skeletal muscles."
Articles about euthanasia:
A Thoughtful Goodbye - Nikki James - www.flyingchanges.com
Euthanasia - How it's done - Habitat for Horses
"If horses don't go to Heaven, then Heaven's no place for me."" We always let the other horses come see the body. They need to do this, to understand what happened. The one time we didn't the horse's mate wandered the pasture for days hunting for her, neighing for hours on end. Let them know what happened. Horses understand more than we give them credit for. They need that few minutes with the body."
Body Disposal
It is illegal in France to bury an animal that weighs more than 40 kg - according to Le Code Rural Article L226-4
Les propriétaires ou détenteurs d’un cadavre d’animal ou d’un lot de cadavres d’animaux pesant au total plus de quarante kilogrammes sont tenus d’avertir dans les plus brefs délais la personne chargée de l’exécution du service public de l’équarrissage d’avoir à procéder à l’enlèvement du ou des cadavres.
Il est interdit par la loi d’enfouir, de jeter en quelque lieu que ce soit ou d’incinérer les cadavres d’animaux ou lots de cadavres d’animaux pesant au total plus de quarante kilogrammes.
Les Haras nationaux - Equarrissage
L'équarrissage, c'est quoi ?
Horses can be cremated following an autopsy at the Laboratoire Départemental d’Analyses et de Recherche de la Haute-Vienne in Limoges. You have to make arrangements to get the body there, at the lab there is equipment to move the body. Reports are that staff are very sensitive, cost for a 500 kg horse in December 2012 was just under 1000 euros for autopsy, private cremation and return of ashes.
According to ANIE, since October 2009 horses can be cremated in France without an autopsy:
Association Nationale pour l'Incinération des Equidés
www.incineris.fr
SERVICE D’INCINÉRATION pour les équidés have 2 centres where equine cremations can be carried out:
Vimoutiers dans l’Orne, Rue des Sorbiers - 61120 Vimoutiers Tél : 02 33 39 80 52
Château-Gaillard dans l’Ain, 255 rue Charles de Gaulle - 01500 Château-Gaillard Tél : 04 74 38 72 22
RESPE
RESPE Réseau d’Epidémio-Surveillance en Pathologie Equine
"The RESPE has four objectives:
1) Insuring a vigilant watch out service for equine illness, in particular those that present important contagious risks and major economical losses or risks to public health. This health surveillance is carried out by four secondary relay services. These are as follows:
- acute respiratory syndrom
- atypical myopathia
- nervous syndrom
- abortion
2) Development of veterinary knowledge and competences allowing the quick collection of accurate epidemiological information which is quickly transferred to the industry
3) Alerting the health authorities, professional and if needed the public health authorities
4) To manage an equine health crisis other than the government regulated diseases (notifiable) through the creation of a competent cellule"
Click here for up to date alerts of contagious diseases
"The RESPE has four objectives:
1) Insuring a vigilant watch out service for equine illness, in particular those that present important contagious risks and major economical losses or risks to public health. This health surveillance is carried out by four secondary relay services. These are as follows:
- acute respiratory syndrom
- atypical myopathia
- nervous syndrom
- abortion
2) Development of veterinary knowledge and competences allowing the quick collection of accurate epidemiological information which is quickly transferred to the industry
3) Alerting the health authorities, professional and if needed the public health authorities
4) To manage an equine health crisis other than the government regulated diseases (notifiable) through the creation of a competent cellule"
Click here for up to date alerts of contagious diseases
Medicines
Information about medicines/drugs and data sheets.
Data sheets for British animal medicines:
http://www.vmd.defra.gov.uk/ProductInformationDatabase/
http://www.noahcompendium.co.uk/Compendium-datasheets_A-Z/Datasheets/-23637.html
Monographs of American veterinary drugs:
http://www.wedgewoodpetrx.com/learning-center/professional-monographs.html
http://www.aavpt.org/DrugMonographs.shtml
SPANA guidelines to certain equine drugs and their use:
http://www.spana-syria.org/download/TB6pharmeng.doc
Information about medicines/drugs and data sheets.
Data sheets for British animal medicines:
http://www.vmd.defra.gov.uk/ProductInformationDatabase/
http://www.noahcompendium.co.uk/Compendium-datasheets_A-Z/Datasheets/-23637.html
Monographs of American veterinary drugs:
http://www.wedgewoodpetrx.com/learning-center/professional-monographs.html
http://www.aavpt.org/DrugMonographs.shtml
SPANA guidelines to certain equine drugs and their use:
http://www.spana-syria.org/download/TB6pharmeng.doc
Blood Testing
Laboratories for equine blood testing in France include:
VetoDiag
Frank Duncombe
Lyon
Cornell University - information about haematology (RBCs, WBCs & platelets) and biochemistry blood testing and more...
http://diaglab.vet.cornell.edu/clinpath/modules/index.htm
Nationwide Laboratories biochemistry interpretation:
http://www.nwlabs.co.uk/testinterp2.htm
Laboratories for equine blood testing in France include:
VetoDiag
Frank Duncombe
Lyon
Cornell University - information about haematology (RBCs, WBCs & platelets) and biochemistry blood testing and more...
http://diaglab.vet.cornell.edu/clinpath/modules/index.htm
Nationwide Laboratories biochemistry interpretation:
http://www.nwlabs.co.uk/testinterp2.htm