
Lyme Disease (borreliosis/borrelia burgdoferi)
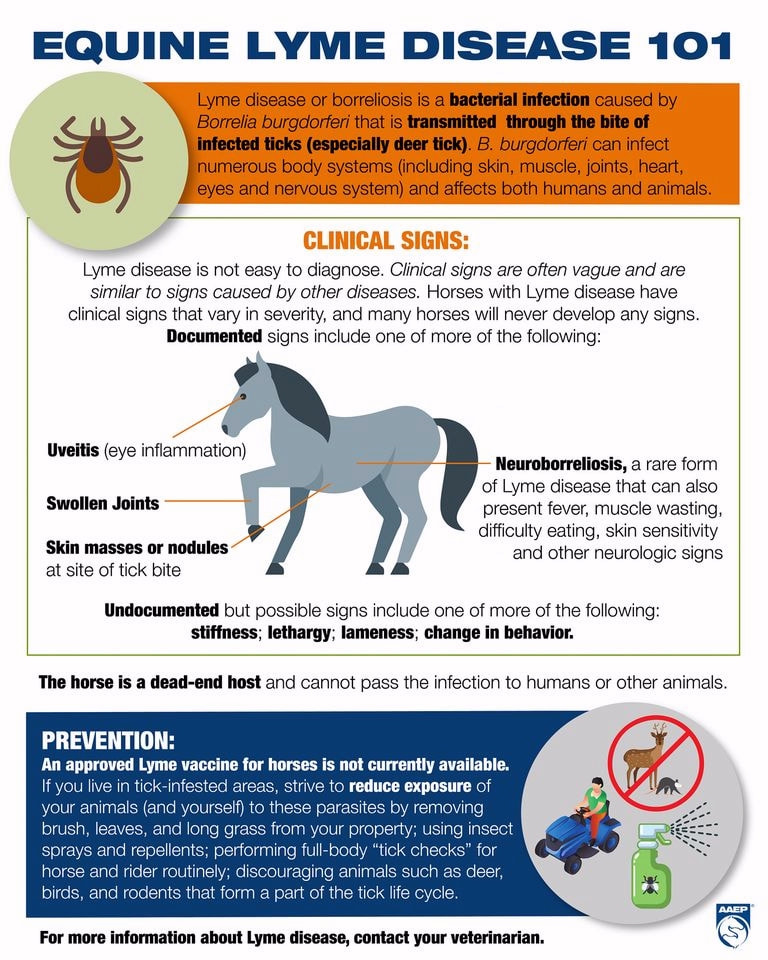
Lyme disease is a tick-borne infectious disease caused by a Gram negative bacteria (spirochaete), Borrelia burgdorferi. It is present in many regions of the UK, Europe and North America, and commonly carried by Ixodes ticks. Exposure to Borrelia burgdorferi is very common in horses living in an endemic area, but Lyme disease in horses, and its prevalence, is not well understood. The bacteria is transmitted when a tick feeds on the blood of a horse, and it is thought that the tick must be attached for several hours for transmission of the bacteria to take place. Ticks may concurrent infect a horse with other diseases such as anaplasmosis or piroplasmosis (PCR testing will generally test for all common tick-borne diseases).
Not all infected horses will develop clinical signs of Lyme disease.
Clinical signs in horses are not well documented but may include:
- stiffness/lameness (often unexplained lameness that may move from leg to leg/sporadic lameness/shifting leg lameness)
- swollen joints
- myalgia (muscle pain/soreness) - may be rapid onset
- hyperaesthesia (abnormal skin sensitivity) - may be rapid onset
- muscle wasting
- changes in behaviour
- neurological signs (e.g. depression, dysphagia (difficulty swallowing/choke), ataxia, head tilting, encephalitis)
- uveitis
- pseudolymphoma/atypical cutaneous nodular lymphoid hyperplasia - skin masses or nodules at the site of a tick bite
- chronic weight loss
Neuroborreliosis is a rare but serious form of Lyme disease with clinical signs that can include fever (but not in all cases), atrophy (wasting) of muscles around the spine, laryngeal dysfunction, dysphagia (difficulty swallowing/choke), facial paresis (inability to move facial muscles), ataxia, skin sensitivity, behavioural changes and neurological signs.
Other reported clinical signs include reluctance to work/poor performance, mild fever, lethargy/depression. Laminitis has been linked anecdotally with Lyme disease, but in the 2018 consensus statement Thomas Divers et al. suggest that there is no evidence of Lyme disease causing laminitis (see below).
Lyme disease is a tick-borne infectious disease caused by a Gram negative bacteria (spirochaete), Borrelia burgdorferi. It is present in many regions of the UK, Europe and North America, and commonly carried by Ixodes ticks. Exposure to Borrelia burgdorferi is very common in horses living in an endemic area, but Lyme disease in horses, and its prevalence, is not well understood. The bacteria is transmitted when a tick feeds on the blood of a horse, and it is thought that the tick must be attached for several hours for transmission of the bacteria to take place. Ticks may concurrent infect a horse with other diseases such as anaplasmosis or piroplasmosis (PCR testing will generally test for all common tick-borne diseases).
Not all infected horses will develop clinical signs of Lyme disease.
Clinical signs in horses are not well documented but may include:
- stiffness/lameness (often unexplained lameness that may move from leg to leg/sporadic lameness/shifting leg lameness)
- swollen joints
- myalgia (muscle pain/soreness) - may be rapid onset
- hyperaesthesia (abnormal skin sensitivity) - may be rapid onset
- muscle wasting
- changes in behaviour
- neurological signs (e.g. depression, dysphagia (difficulty swallowing/choke), ataxia, head tilting, encephalitis)
- uveitis
- pseudolymphoma/atypical cutaneous nodular lymphoid hyperplasia - skin masses or nodules at the site of a tick bite
- chronic weight loss
Neuroborreliosis is a rare but serious form of Lyme disease with clinical signs that can include fever (but not in all cases), atrophy (wasting) of muscles around the spine, laryngeal dysfunction, dysphagia (difficulty swallowing/choke), facial paresis (inability to move facial muscles), ataxia, skin sensitivity, behavioural changes and neurological signs.
Other reported clinical signs include reluctance to work/poor performance, mild fever, lethargy/depression. Laminitis has been linked anecdotally with Lyme disease, but in the 2018 consensus statement Thomas Divers et al. suggest that there is no evidence of Lyme disease causing laminitis (see below).
Source: AAEP September 2020
Definitive diagnosis of Lyme disease is complicated. Diagnosis is based on exposure to B. burgdorferi, cytology or histopathology of infected fluid or tissue and antigen detection. Tests used include PCR (can confirm active infection) and ELISA (confirms antibody production but not current infection). Cornell in the USA offers a multiplex test that can distinguish the different stages of the immune response and thereby indicate whether a horse has a current or previous infection.
Same day PCR testing is carried out at Equisyn Equine Vet Clinic near 16260 Chasseneuil-sur-Bonnieure. The PCR profile run is the Piro-Like/tick-borne disease profile also run by Frank Duncombe/Labeo, supported by Labeo, and includes Lyme disease, anaplasmosis, both forms of piroplasmosis and leptospirosis. PCR testing is available to non-clients as well as clients of the clinic.
Other laboratories in France that test for Lyme disease include Frank Duncombe/Labeo and Vetodiag.
PCR (polymerase chain reaction) looks for and confirms the presence of parasite DNA and is considered highly specific and sensitive. PCR can detect low levels of parasitic infection and can be used for chronic infections.
Other laboratories in France that test for Lyme disease include Frank Duncombe/Labeo and Vetodiag.
PCR (polymerase chain reaction) looks for and confirms the presence of parasite DNA and is considered highly specific and sensitive. PCR can detect low levels of parasitic infection and can be used for chronic infections.
Same day PCR testing is offered by Equisyn vets at Chasseneuil-sur-Bonnieure - the same tick-borne PCR profile offered by Labeo/Frank Duncombe, supported by Labeo. Local vets can take/send blood to Equisyn for PCR testing to speed up results.
|
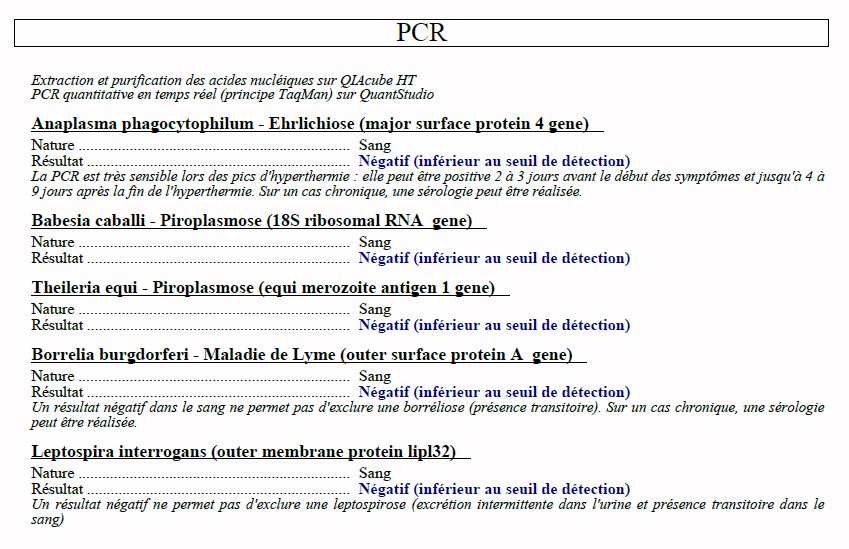
Results of a "piro-like" PCR profile that tests for anaplasmosis, both forms of piroplasmosis, Lyme disease and leptospirosis.
|
Treatment of Lyme disease in horses is with antibiotics - oxytetracycline and doxycycline have been used. The duration of treatment is not well defined but may be one week of antibiotics in acute cases and up to one month in chronic cases. Antibiotics should only be used for horses with clinical signs and positive blood results. NSAIDs may be used e.g. for horses with lameness or swollen joints.
There is currently no Lyme disease vaccine for horses. Some vets have given Lyme vaccines licensed for dogs to horses, but research (Guarino et al. 2017) suggests that Lyme vaccines for dogs give only short-term antibody responses in horses, and these may be of low magnitude.
Prevention involves ensuring horses' exposure to ticks is minimized (e.g. by keeping horses away from long grass), and that horses are checked at least daily for ticks and any ticks found are removed carefully, as prompt removal of ticks should reduce the risk of infection.
AAEP Infectious Disease Guidelines: Borrelia burgdorferi infection and Lyme disease 2020
Equine Lyme Disease (borreliosis) - EDCC AAEP 2020
Is it Lyme Disease? Jean-Yin Tan, thehorse.com March 2020
Divers TJ, Gardner RB, Madigan JE, Witonsky SG, Bertone JJ, Swinebroad EL, Schutzer SE, Johnson AL
Borrelia burgdorferi Infection and Lyme Disease in North American Horses: A Consensus Statement
J Vet Intern Med. 2018 Mar-Apr; 32(2): 617–632. Published online 2018 Feb 22. doi: 10.1111/jvim.15042
"Although anecdotal, web‐based, reports of equine Lyme disease causing laminitis, headshaking, hepatitis, nephritis, or fistulous withers can be found, there is little research and no overt clinical data to support the claims. The range of specific clinical signs associated with Lyme disease is certainly in need of further experimental and epidemiological evaluation, but future progress might well be on a case by case report basis. The best—documented, naturally occurring syndromes attributed to B. burgdorferi infection include neuroborreliosis, uveitis, and cutaneous pseudolymphoma. The association of B. burgdorferi infection with stiffness and lameness in horses is not well documented and there is no evidence of the infection causing laminitis."
An update on Borrelia burgdorferi - Jamie Prutton, Veterinary Practice May 2018
Lyme Disease and Anaplasmosis - Liphook Equine Hospital (2016)
[Copied from Horse Nutrition and Health, a website available to Friends of The Laminitis Site, with permission of the author Andrea Jones/The Laminitis Site).
Information is given as a guide only and must not be relied upon. Please consult your vet for all equine medical matters.